By Allison Sikorsky, PMHNP
For years, I thought documentation was the problem. Like many psychiatrists, PMHNPs, and therapists, I spent evenings finishing notes and weekends catching up on charts, spending far too much time thinking about documentation when I wasn’t at work.
When I began building PMHScribe and talking with more behavioral health providers across the country, I expected to hear the same thing over and over: “I hate charting.”
Instead, I heard something different.
Providers weren’t really talking about documentation.They were talking about exhaustion, feeling mentally drained at the end of the day, and never feeling caught up. They were talking about carrying work home, even when their laptop stayed at the office. That’s when I realized something important: The documentation problem isn’t really documentation.
Documentation is simply where the burden shows up.
The real issue is that behavioral health providers carry multiple types of burden throughout the day, and documentation often becomes the place where those burdens collide.
Behavioral health providers don’t simply document symptoms and treatment plans. Every day, psychiatrists, PMHNPs, therapists, and behavioral health teams move between stories that require attention, empathy, memory, judgment, and emotional presence. A provider may spend a single day discussing:
Each encounter requires thoughtful clinical documentation. But before documentation ever begins, providers have already spent hours listening, assessing, interpreting, supporting, and making decisions.
By the end of the day, most providers aren’t tired because they have notes to write. They’re tired because they’ve been carrying so much.
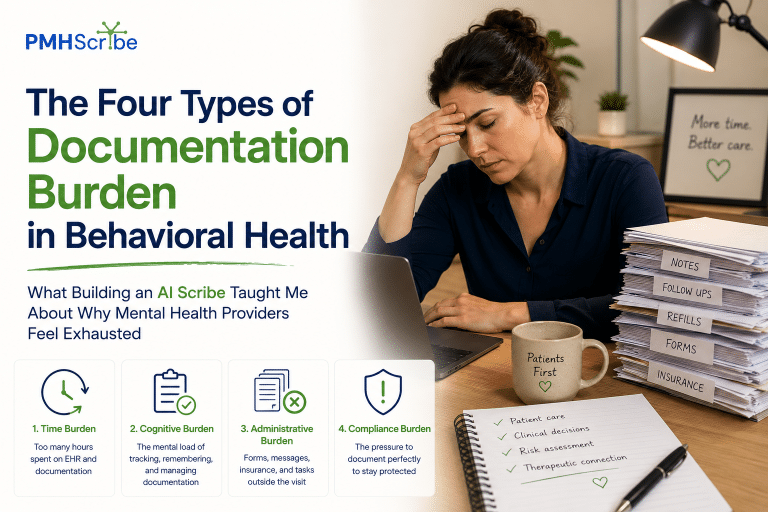
Over time, I’ve come to think about documentation burden differently. What we often call “documentation burden” is actually four separate challenges happening simultaneously.
This is the burden everyone notices first. It’s the unfinished notes waiting at the end of the day. The hour spent charting after dinner. The Saturday morning spent catching up because the week moved too quickly.
Most conversations about AI scribes focus here, and understandably so. Time matters, but time is only one piece of the equation.
This is the burden that often goes unnoticed. Behavioral health providers spend their entire day holding information.
Who started a new medication, who reported worsening symptoms, who disclosed a traumatic event, and who needs follow-up, who is improving.
Who is struggling.
The challenge isn’t simply documenting the encounter. The challenge is remembering and organizing dozens of complex patient narratives throughout the day. Many providers aren’t exhausted from typing, they are exhausted from thinking.
Behavioral health is deeply human work. Mental health providers spend their days sitting with grief, trauma, anxiety, addiction, crisis, uncertainty, and loss.
Those experiences don’t disappear when the session ends. Even the most experienced clinicians can feel the weight of difficult conversations and difficult decisions. When providers talk about burnout, documentation is often part of the discussion.
But emotional burden is frequently sitting just beneath the surface.
Then there is everything else.
Treatment plans.
Compliance requirements.
Insurance documentation.
EHR workflows.
Prior authorizations.
Clinical standards.
Reporting requirements.
The note itself is often only one small piece of a much larger administrative system that providers must navigate every day.
When providers search for:
I don’t think they’re really asking about software, I think they’re asking a much more important question:
A documentation platform that only generates notes faster may help reduce time burden. A documentation platform that fits naturally into behavioral health workflows can help reduce cognitive burden as well.
The most valuable technology isn’t the technology that feels impressive, it’s the technology that removes friction.
Behavioral health documentation requires a level of nuance that is difficult to appreciate unless you’ve done the work yourself. Providers may be documenting:
Unlike many areas of healthcare, context matters enormously. A note is often more than a record of symptoms. It’s a clinical narrative that helps explain where a patient has been, where they are today, and where treatment is headed next.
This is one reason many providers specifically search for an AI scribe for psychiatry, PMHNP practice, therapy, or behavioral health rather than a generic medical AI scribe.
Yes.
Many therapists, psychiatrists, and PMHNPs now use AI-assisted documentation tools to help organize information and generate draft notes. However, the goal should never be to replace clinical judgment.
Technology can help reduce administrative work. It cannot replace therapeutic relationships, empathy, clinical expertise, or professional decision-making.
The provider remains the clinician.
AI simply helps lighten the workload.
The best AI scribe for behavioral health providers is one that understands behavioral health. That sounds obvious, but it’s important. Psychiatrists and PMHNPs need documentation tools that support:
The goal isn’t just creating notes faster, the goal is creating a workflow that feels sustainable.
I don’t believe the future of behavioral health documentation is about creating more technology, I believe it’s about creating less burden. The most valuable tools won’t necessarily be the ones with the most features. They’ll be the ones that help providers spend less time managing documentation and more time caring for patients.
Because ultimately, the documentation problem isn’t really documentation. It’s that too many mental health providers never get the chance to feel finished.
And helping providers reclaim that feeling may be one of the most important opportunities AI has to offer behavioral healthcare.
Allison Sikorsky, PMHNP is a practicing Psychiatric Mental Health Nurse Practitioner and founder of PMHScribe. Through her clinical work, she experienced firsthand the documentation burden facing behavioral health providers and became passionate about helping clinicians reduce administrative workload while maintaining high-quality patient care.